what has led to the growth of the amblance services industry in the last five years
The ambulance service plays a unique role. As a fundamental part of the country's emergency services, ambulance trusts operate alongside the police and fire service in addition to the balance of the NHS, and the wider wellness and care system.
At a national level, ambulance operation is monitored past the time it takes the service to respond to different levels of emergency intendance. The largest academic study into ambulances in the world, and all-encompassing piloting with the sector, resulted in the ambulance quality standards being updated in 2017. This prioritised the sickest patients, ensuring they receive the fastest response, drove clinically and operationally efficient behaviours and put an end to unacceptably long waits by ensuring that resources are distributed more equitably across all patients.
The ambulance service has at present operated for 18 months under the new framework, pregnant we now have plenty information to expect at trends and proceeds a deeper understanding of performance.
The ambulance service plays a unique office. As a key part of the country'southward emergency services, ambulance trusts operate alongside the police force and fire service in improver to the residual of the NHS, and the wider health and care system.
Assay manager
An expanding service
In that location are 10 ambulance trusts across England. Each trust covers a large geography, roofing multiple local integrated systems which include numerous hospitals with A&Due east departments and varying community, principal and social intendance provision and support millions of people.
There is a common misconception that an ambulance is but 'a blue light taxi' or that ambulances are staffed by paramedics whose main job is to transport someone to hospital. This narrow understanding of what the ambulance service does fails to reflect the broad and evolving role the service has to play within health and intendance systems, particularly as services become more integrated. I challenge for the NHS is to try to shift public perception and increase understanding of the important role ambulance services tin can play as a front door to the NHS (particularly given many ambulance trusts also manage the NHS 111 service), in signposting and referring frequent and vulnerable patients to other services, and in delivering clinical treatment and care.
Ambulance trusts provide a range of services including;
- handling 999 calls
- co-ordinating and dispatching ambulances
- providing clinical interventions on the scene for seriously ill patients and transporting people to hospital in an emergency
- referring patients onto culling services across health and intendance
- multidisciplinary response teams e.grand. paramedic, mental health nurse and constabulary responses to those in mental wellness crisis or consultant-led response vehicles to cardiac arrests
- see and treat – when a person does not require hospital care simply instead a paramedic or another clinician provides treatment at the scene, which could be in someone's home or in the customs
- Hear and treat – when a person does not require an ambulance but a clinician is able to provide treatment and advice over the phone
- Hospital transportation to help with hospital transfers and discharges
- Some ambulance services are also commissioned to provide NHS 111 services that provide advice over the telephone and increasingly are able to volume appointments in GP surgeries or urgent care centres.
One challenge for the NHS is to try to shift public perception and increase understanding of the of import role ambulance services can play as a front door to the NHS, in signposting and referring frequent and vulnerable patients to other services, and in delivering clinical treatment and care.
Assay director
The sometime national ambulance standards
Prior to the introduction of the new national ambulance quality standards, ambulance performance was measured by two response time targets:
- 75% of category A (immediately life-threatening) calls should receive a response within eight minutes
- if a category A patient requires ship, this should go far within xix minutes of the request for transport being made, 95% of the time.
From June 2013, the erstwhile category A call category was further separated into Ruby one and Scarlet 2 calls:
- red i calls were the most fourth dimension critical and covered cardiac abort patients who were not animate and did non have a pulse, and other severe weather.
- ruby-red two calls were serious just less immediately fourth dimension critical and covered weather condition such as stroke and fits.
Post-obit calls from paramedics to review ambulance response times that were developed in the 1970'southward, the NHS embarked on a review setting upward the ambulance response programme (ARP) in 2015. The objectives of the review were:
- Prioritising the sickest patients, to ensure they receive the fastest response.
- Driving clinically and operationally efficient behaviours, so the patient gets the response they demand first time and in a clinically appropriate timeframe.
- Putting an end to unacceptably long waits by ensuring that resource are distributed more deservedly amongst all patients.
Following calls from paramedics to review ambulance response times that were developed in the 1970's, the NHS embarked on a review setting up the ambulance response programme (ARP) in 2015.
Analysis director
The review made changes to the 999 script to aid with early recognition of life threatening conditions, in particular cardiac arrests. In improver, revisions were made to the call categories – resulting in a new triaging procedure that ranks the severity of the call and allows for more constructive prioritisation.
The changes were piloted with two ambulance services in England and the Academy of Sheffield carried out a big scale written report in which over fourteen million 999 calls handled with the new 999 script were reviewed over an 18 month period. The roll out of the new operational model was and so staggered across different ambulance services with them now all working within the new framework.
The new ambulance standards
The new ambulance standards are different to the previous targets in a few ways.
Firstly, the targets employ to all calls and not just a proportion of calls, raising the standard beyond the lath. Secondly, the average fourth dimension for responding to those in life threatening weather condition has fallen from eight minutes, down to 7 minutes. And thirdly, there are targets for the xcth percentile. This indicate may be harder to interpret to the public but what information technology does is ensure that calls which have missed the boilerplate response target are nonetheless responded to in a timely manor. Lastly, the changes mean that the service can dispatch the right vehicle first time and in cases such every bit strokes or cardiac arrests, tin can focus on taking patients to specialist hospitals so they tin can receive the best care.
All these changes are aimed at providing a more effective and safer service overall for the public.
Table one: Ambulance quality standards
Electric current performance
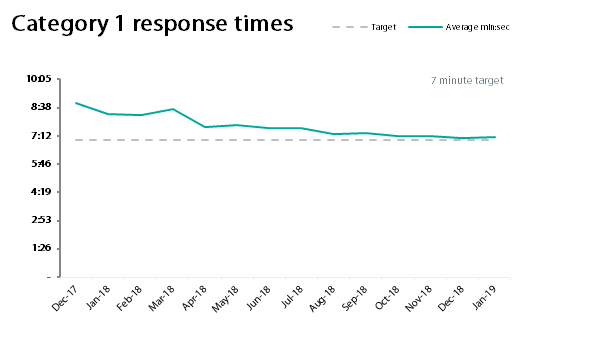
Since the introduction of the new standards, trusts have improved performance moving closer to the targets. Particular progress has been made in relation to category 1 calls.
In January 2019, 6 out of the 10 trusts exceeded the target for category 1 calls. Nationally, the average response fourth dimension was 7:08mins – eight seconds over the target. The average 90thursday percentile response time was 12:20 minutes; 2 minutes and 40 seconds quicker than the target.
As shown in figure one, national performance has been improving since the new standards were introduced.
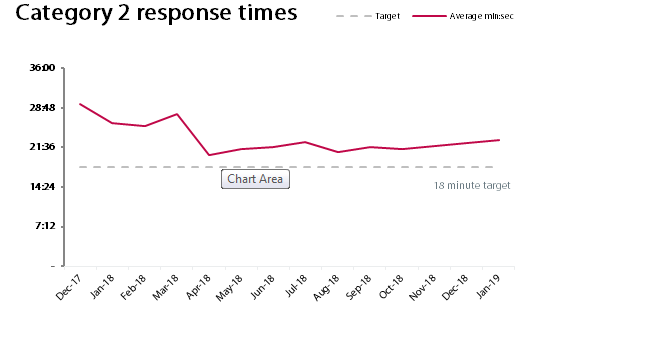
The national average response time for category 2 was 22:58 minutes in January 2019. Functioning against the category 2 response times is more varied, with only 2 trusts exceeding the target. The deviation betwixt the shortest and longest response time is over 18 minutes – same equally the average response time target for category 2. Instead of being quick to criticise the ambulance service for current performance, we must be cognisant that it was e'er going to have time, investment and additional staff to evangelize the quality standards across the board.
Current challenges for the ambulance sector
Similarly to the remainder of the health and care sector, the ambulance service has struggled due to large increases in demand, a lack of funding and widespread workforce shortages. The service experiences higher levels of sickness absence than other services and ambulance staff are more likely to be physically assaulted or experience verbal abuse when working.
Whilst demand, money and recruitment and retention challenges are in some style consistent across ambulance trusts, there are a range of factors that tin impact the operational model and functioning of an ambulance service.
In that location is variation in terms of:
- the size of the dissimilar geographies
- population count
- population profile – in particular around age
- how rural or urban the geography i.e. spread of densely populated cities and more sparsely populated areas
- the number and spread of A&Eastward departments
- the different health and intendance systems due east.g. the number and blazon of specialist services, the functioning and period in local acute hospitals
- the quality of community services, care homes and primary care
- other emergency services including the fire service and police force service.
A number of these factors are related to the demand and quality of other NHS services – things that are often out of the ambulance service's control.
One of the most challenging things for ambulance trusts in terms of planning and deployment of vehicles is when staff and vehicles are held upwards handing patients over to astute hospitals. These 'handover delays' happen when hospitals are running at capacity and there are no beds available. These delays result with the take chances to patients existence extended from the hospital, out into the community, as ambulances are unable to be re-deployed to people waiting for an ambulance; meaning people have to await longer due to other parts of the health system.
Similarly to the residue of the health and intendance sector, the ambulance service has struggled due to large increases in demand, a lack of funding and widespread workforce shortages. The service experiences higher levels of sickness absence than other services and ambulance staff are more likely to be physically assaulted or experience verbal abuse when working.
Analysis manager
The direction of travel
Despite demand for ambulances increasing significantly in the terminal yr, there has been a range of developments in conjunction with the new quality standards which would point that functioning of the sector may amend over the next few years.
Funding
In the center of 2018 the government appear an investment of £36.3m in the ambulance service for the 70th birthday of the NHS. The investment will provide 256 state of the art ambulances as well as providing some trusts with coin to grow their workforce to help them meet the growing need for their services.
Workforce
To boost recruitment, the sector has expanded the training routes to qualify as a paramedic, including paramedic courses, a degree in paramedic science and apprenticeship degrees. In 2018 information technology was also appear that paramedics will be eligible to train equally independent and supplementary prescribers, diversifying and unlocking the potential of the ambulance service. New intendance models and the development of more than integrated ways of working between community and primary care services may also open up upwardly new partnerships for ambulance staff to support these endeavours.
There was also good news in the 2019 NHS staff survey for the ambulance service, which could be positive in terms of retentivity. The ambulance service continues to struggle with staff engagement indicators, existence worse than in whatsoever other sector in the NHS, simply the service bucked the downward trend and has seen twelvemonth on year improvements recently.
Despite demand for ambulances increasing significantly in the last year, at that place has been a range of developments in conjunction with the new quality standards which would bespeak that performance of the sector may improve over the side by side few years.
Analysis manager
Organization working
Ambulance trusts play a unique role in local health and care systems. Covering multiple systems with varying degrees of maturity, they can offer a joined upwards perspective at a regional level.
Increased system working, new care models and a system focus on fugitive costly inpatient intendance have already seen an expansion of the role of the ambulance service in some regions.
As need for the NHS continues to rise we must recognise the potential the ambulance service offers in helping keep people out of hospital.
The long term plan plans for the sector are encouraging with cardinal changes effectually emergency mental health intendance provision to be rolled out across ambulance trusts. For those that are deputed to provide a NHS 111 service, volition be expected to work with systems to ensure that NHS 111 is the primal indicate of contact for those experiencing a mental health crisis inside the next 10 years.
Equally demand for the NHS continues to rise we must recognise the potential the ambulance service offers in helping keep people out of hospital.
Analysis manager
Determination
The outlook for the ambulance service is positive with improved staff engagement and morale an important marker for the direction of travel, alongside renewed focus on ambulance services playing a cardinal function equally 'an integrator' within local systems.
The recent review of response targets has been cornerstone for change. Sufficient investment, growing the workforce, and upgrading the fleet of ambulances will help trusts proceed to make progress confronting the new quality standards.
Meanwhile, as the NHS carries out a clinical review of targets in acute care, national policy leaders need look no farther than the review of the ambulance quality standards equally a template. Clinically led, the review team placed patient safety was of paramount importance - extensive piloting prior to coil out, rigour and full engagement with trusts are all success criteria that should be shared and replicated.
Source: https://nhsproviders.org/the-ambulance-service-understanding-the-new-standards
0 Response to "what has led to the growth of the amblance services industry in the last five years"
Post a Comment